

If you've been reading about SGLT2, you've probably been wondering about its role in the body. This article will explain the function of SGLT2 and its potential side effects. In addition, you'll learn what drugs inhibit SGLT2 transport. You can also learn about the pharmacology of these drugs. But before you begin your treatment, be sure to read about SGLT2 transport and function.
Table of Contents
SGLT2 transport
SGLT2 is a phospholipase B that plays a critical role in the synthesis of the lipid soluble peptide glutathione. The enzyme is a major player in the regulation of glucose levels in the blood and in the body. Its transport stoichiometry is two Na+ for each glucose. Electrophysiological measurements and radiotracer flux studies have demonstrated that SGLT1 functions as a Na+ uniporter in the absence of glucose and is also capable of passively transporting water. Na+ uniportation requires conformational changes within the transporter, and water permeation shows behavior similar to that of water channels. It is also independent of glucose and Na+ concentration gradients, and is inhibited by phlorizin.
SGLT3 transport has been studied in rat kidneys. One study focused on determining its substrate selectivity. The authors showed that glucose and a-MG induced low-affinity currents in a Na+-dependent manner. The reversible nature of the currents also confirmed their substrate selectivity. Moreover, the enzyme was found to enhance glucose transport in the presence of Na+ and pH levels.
Interestingly, SGLT2 is expressed in the proximal tubule of the kidney. Its distal straight part of the proximal tubules expresses SGLT2 and MAP17. Moreover, the expression of both proteins increased SGLT2 transport activity significantly. Furthermore, mice that lack SGLT2 and MAP17 had decreased glucose reabsorption. In contrast, wild-type mice reabsorb 90% of the filtered glucose. Interestingly, the two proteins are not completely redundant.
The regulation of SGLT2 in T2D has been studied in Zucker rats. Obese Zucker rats express higher levels of SGLT1 and SGLT2 mRNA than lean Zucker rats. A human study has also used urine from patients with T2D to study its expression. Interestingly, SGLT2 mRNA and protein levels were significantly higher in diabetic patients than in controls. The increased expression of GLUT2 increases glucose uptake in diabetic patients.
To further study the expression of SGLT2 in human cells, we used a plasmid carrying a V5 N-terminal modification of the gene. The plasmid produced a similar size band to pcDNA3.1 HA23MAP17. However, the V5 N-terminal modification of the gene was used in this experiment to identify a specific fusion protein that is expressed in human cells.
Function
The mechanism by which SGLT2 is regulated in the kidney is unclear. There are a number of different cellular pathways that may affect the protein, but the role of vascular shear stress is a likely factor. However, SGLT2 inhibition in cultured human coronary VSMCs may differ from that of VSMCs from the mesenteric arteries. Further studies are needed to better understand the function of SGLT2.
The mutant SGLT2 631 K-GFP fusion protein inhibited SGLT2 activity, resulting in a 0.285-fold reduction in Xanthine dehydrogenase/oxidase expression. This resulted in a decrease in the uptake of glucose analogs. Therefore, a better understanding of SGLT2's role in glucose transport in the body is needed to develop anti-diabetes drugs.
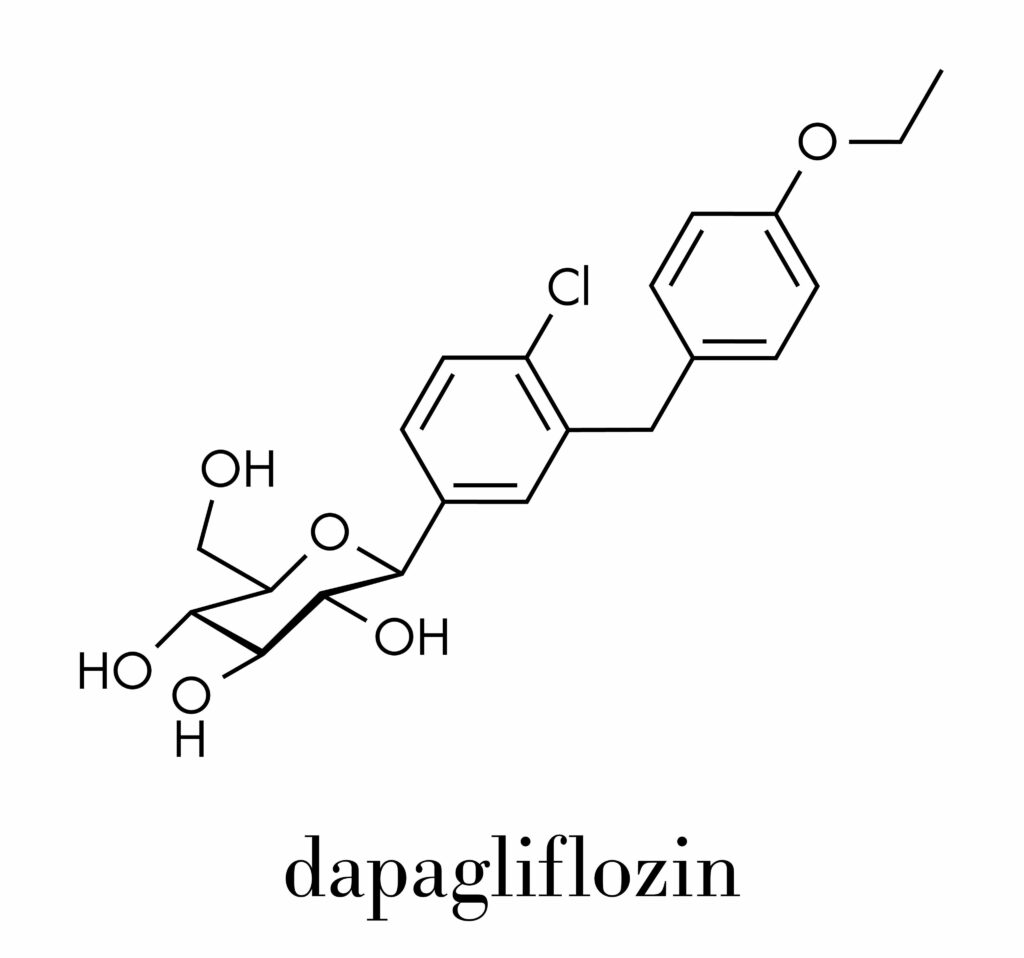
In rats with HF, the SGLT2 inhibitor dapagliflozin increased renal excretory responses, which are related to elevated expression of SGLT2 in the kidneys. However, acute inhibition of SGLT2 did not affect renal sodium excretion, arterial blood pressure, or HR, suggesting that the response to SGLT2 inhibition in HF is due to a reduction in fluid.
The SGLT2 inhibitors significantly reduced cardiovascular mortality, including nonfatal myocardial infarction. They reduced the risk of acute kidney failure, lowered the progression of chronic kidney disease, improved urinary albumin creatinine ratio, and improved glomerular filtration rate in long-term treatments. These effects may explain the increasing prevalence of chronic kidney disease in the United States. However, more research is needed to determine their efficacy and safety in these patients.
The sodium-glucose cotransporter 2 (SGLT2) is a protein located in the proximal tubules of the kidney. This protein is implicated in approximately 90% of reabsorbed glucose in the body. Increasing the activity and expression of SGLT2 can cause complications, including diabetes mellitus. SGLT2 inhibitors can protect kidneys from the effects of hyperglycemia and promote glucose excretion.
SGLT2 inhibitors are widely used to treat diabetes and have been clinically shown to improve food intake. However, its role and presence in the central nervous system (CNS) remain unclear. Therefore, this study aimed to elucidate the possible functions of SGLT2 in the CNS and identify its effects. The results of this study indicate that a novel drug targeting the SGLT2 pathway may improve the health of people with diabetes.
Side effects

Patients who are taking an SGLT2 inhibitor should be aware of potential side effects, especially those involving blood sugar. A high level of glucose in the bloodstream may cause a condition known as diabetic ketoacidosis, a potentially life-threatening condition characterized by nausea, vomiting, diarrhea, confusion, trouble breathing, and unusual fatigue. If the condition is not treated quickly, the patient may develop severe complications and even die.
SGLT2 inhibitors can increase the risk of bacterial infections, particularly in the genital area. This can lead to serious complications such as necrotizing fasciitis and Fournier's gangrene, which are caused by flesh-eating bacteria. Other potential side effects include urinary tract infections and yeast infections. However, there are some precautions patients should take to minimize their risk of developing these complications.
One side effect of an SGLT2 inhibitor is increased urination, which can lead to dehydration. Those with kidney problems or high potassium levels should not take these medications. These drugs can also increase the risk of kidney failure. Furthermore, they can also cause low blood sugar, which can lead to weight loss. This is because glucose contains calories. Hence, people with kidney problems and active bladder cancer should avoid taking them.
A patient with FRG should consult a physician to discuss the risks. Generally, elevated uric acid levels may be associated with worse outcomes. However, it remains unclear how SGLT2 inhibitors can promote hypouricaemia. In general, however, SGLT2 inhibitors are safe for long-term use. The risk of hypoglycemia can be minimized by reducing the amount of sugar in the urine.
The SGLT2 inhibitors are a new class of drugs for type 2 diabetes. They lower blood sugar by increasing the excretion of glucose in the urine and decreasing reabsorption in the kidney. This occurs independent of insulin concentrations. Patients who have high blood sugar can use SGLT2 inhibitors alone or with other diabetic medications. These drugs are available in over the counter forms and can be prescribed with or without a doctor's prescription.
Pharmacology

The International Journal of Molecular Sciences is devoted to studies of SGLT2is in human physiology and disease. Original investigations, particularly those with solid basic/molecular research foundations, are especially encouraged. Short communications and review articles are also welcome. Pure clinical investigations are not appropriate for submission. Please refer to the journal's Author Guidelines for more information. To submit an article, please follow the guidelines below:
SGLT2 inhibitors cause significant BP reductions, with systolic BP lowered by 1.66 to 6.9mmHg and diastolic BP reduced by 0.88 to 3.5mmHg. In addition, SGLT2 inhibitors have no hyponatremia. Initial BP reduction is attributed to diuretic and volume-depletion effects, but longer-term effects are mediated by inhibition of the renin-angiotensin system. Hence, they are a good option for patients with type 2 diabetes.
A common side effect of SGLT2 inhibitors is increased risk of myalgia. Nevertheless, these complications are rare and the drug can be used for short periods. Pharmacological trials are ongoing to determine long-term safety of these inhibitors. They may cause adverse side effects such as hypoglycemia and DKA, but they can also prevent kidney failure. These side effects may require pharmacovigilance.
Inhibitors of SGLT2 function via a novel mechanism in the kidneys that inhibit renal tubular glucose reabsorption. These inhibitors decrease blood glucose without stimulating insulin secretion or b-cell function. This makes SGLT2 inhibitors an appealing option for people with diabetes who cannot tolerate insulin or have acceptable risk factors. There is also evidence of positive cardiovascular effects of SGLT2 inhibitors. Further studies are needed to establish long-term efficacy.

Recent Post







